|
|
Liver Metastases
General Considerations
- In this country, a focal liver lesion is less likely to represent a primary malignancy than a metastasis
- Metastasis is the most common neoplasm in an adult liver
- Only lymph nodes harbor more metastatic deposits than the liver
- The liver is a principle target for gastrointestinal malignancies
- The most common primary sites for metastatic lesions to the liver in adults are:
- Colon
- Stomach
- Pancreas
- Breast
- Lung
- Eye
- In children, most common primary sites for metastatic lesions to the liver are:
- Neuroblastoma
- Wilms tumor
- Leukemia
- Most liver metastases are multiple
- Multiple lesions often vary in size suggesting tumor seeding which occurs episodically
- About ½ of patients with liver metastases have clinical signs of hepatomegaly or ascites
- Liver function tests tend to be insensitive and nonspecific
- Almost all tumors that metastasize to the liver also metastasize elsewhere at the same time
- Some tumors, such as colon carcinoma, carcinoid, and hepatocellular carcinoma (HCC) may present with lesions confined to the liver
Pathologic characteristics of metastases
- The pathology of metastatic deposits in the liver closely resembles the primary tumor, i.e. they are usually as vascular as their primary tumors
- In general, most metastases are hypovascular, but some primaries characteristically have hypervascular metastases
- Hypervascular metastases
- Carcinoids
- Leiomyosarcomas
- Neuroendocrine tumors
- Renal carcinomas
- Thyroid carcinomas
- Choriocarcinomas
- Occasionally pancreas, ovary, or breast
- Blood flow increases in all metastases, even hypovascular tumors
- Neovascularity, vascular encasement, and arteriovenous shunting are rare
- Large metastases can outgrow their blood supply leading to central necrosis
Blood flow of the Liver
- The liver has a dual blood supply from both the hepatic artery (25% of the flow) and portal vein (70% of hepatic blood flow)
- Arterial blood is carried by the hepatic artery
- Portal vein drains venous blood from the GI tract and other parts of the splanchnic area
- Portal venous blood supplies about 50-60% of the liver’s oxygen requirement
- Remainder from hepatic arterial flow
- Venous drainage from the liver is by the hepatic veins and the small veins directly from the caudate lobe to the inferior vena cava (IVC)
- The hepatic veins drain via the IVC to the right atrium
Imaging Findings in Liver Metastases
- Conventional radiographs play little role in the diagnosis of liver metastases
- A plain radiograph of the abdomen may suggest hepatomegaly or ascites
- Calcified metastases can occur from several primary sites, usually a mucin-secreting ovarian or colorectal cancer
- Calcification within metastases tends to be amorphous
- For more on calcified liver metastases, see this link

CT findings
- CT is the study of choice for evaluating liver metastases
- CT is the most sensitive technique for the detection of liver metastases (80-90% sensitivity and 99% specificity for contrast-enhanced scans)
- Most liver metastases are hypovascular compared with surrounding parenchyma and therefore most lesions appear either hypoattenuating or isoattenuating relative to the surrounding normal liver
- Most studies of the liver for metastatic disease are contrast-enhanced
- Hypovascular lesions are more easily detected using contrast-enhancement
- On contrast-enhanced scans, liver metastases may display slight peripheral enhancement with a hypoattenuating center
- The margin of the lesions can vary from well defined to ill defined
- Hyperattenuating lesions are uncommon
- On the portal venous phase of scanning, some highly vascular primary tumors such as renal cell carcinomas, pancreatic islet cell tumors, pheochromocytomas, melanomas, and breast carcinomas, may appear as isoattenuating to normal liver
- Multiple hemangiomas can be mistaken for metastases
- Cysts show no enhancement
- Focal nodular hyperplasia (FNH) -- may look like vascular metastases
- Focal fatty sparing in a diffusely fatty liver can simulate metastases
MRI findings
- MRI is usually used as a as problem-solving rather than a primary technique in the diagnosis of liver metastases
- Most liver tumors, benign or malignant, appear as hypointense lesions on T1-weighted images and hyperintense lesions on T2-weighted images
- Gadolinium-enhanced MRI improves both the detection of focal liver masses and the differentiation of benign from malignant lesions
- Hemangiomas are reliably diagnosed with MRI
General US findings
- US appearance of liver metastases is nonspecific
- Hepatomegaly
- The liver surface may appear nodular or lobular
- Multiple hepatic nodules of different sizes within the liver is nearly always due to metastases


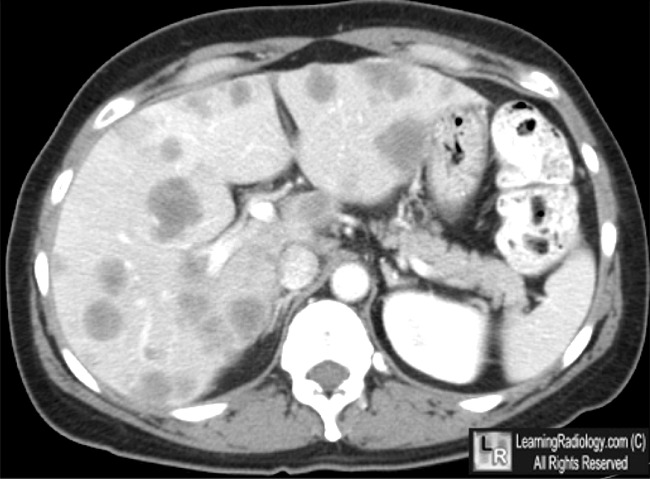
Liver metastases, contrast-enhanced CT. Multiple hypoattenuating lesions of varying sizes are seen
in both the left and right lobes of the liver, some with indistinct margins.
The patient had colorectal carcinoma.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon
Liver Metastases eMedicine Ali Nawaz Khan, MBBS, FRCP, FRCR with Sumaira Macdonald, MBChB, MRCP, FRCR, PhD and Ajay Pankhania, MBChB, MRCS and David Sherlock, MBBS, FRCS
|
|
|

{kind=link}
{kind=link}